 This information is intended for healthcare professionals based in Ireland.
If you are not a healthcare professional in Ireland, click here
This information is intended for healthcare professionals based in Ireland.
If you are not a healthcare professional in Ireland, click here
This information is intended for healthcare professionals based in Ireland.
If you are not a healthcare professional in Ireland, click here
AUGUSTUS Clinical Trial
In the AUGUSTUS clinical trial, ELIQUIS demonstrated superiority over VKA for major or CRNM bleeding in patients with NVAF after a recent ACS and / or PCI1,2*
- Eliquis showed overall superiority to VKA in the study population. For VKA, additional analyses using subgroups by TTR showed highest bleeding associated with the lowest quartile of TTR and similar bleeding rates in the highest quartile of TTR vs Eliquis1
- Eliquis should be used with caution when coadministered with aspirin and/or P2Y12 inhibitors because these medicinal products typically increase the bleeding risk. In patients with AF and conditions that warrant mono or dual antiplatelet therapy, a careful assessment of the potential benefits against the potential risks should be made before combining this therapy with Eliquis2
- There is limited experience of treatment with ELIQUIS at the recommended dose for NVAF patients when used in combination with antiplatelet agents in patients with ACS and / or undergoing PCI after haemostasis is achieved2
 Discover the data on the safety outcome of ELIQUIS in patients with NVAF after a recent ACS and / or PCI
Discover the data on the safety outcome of ELIQUIS in patients with NVAF after a recent ACS and / or PCI
Watch the video below to learn how the AUGUSTUS trial may support your treatment decisions in patients with NVAF after a recent ACS and / or PCI1
This is a promotional video created by the BMS / Pfizer Alliance
What were the study hypotheses?
The 2 x 2 factorial design allowed for the evaluation of two independent study hypotheses:1
- Non-inferiority and possible superiority of ELIQUIS vs. VKA, each in combination with a P2Y12 inhibitor with / without aspirin for the outcome of ISTH major or CRNM bleeding
- Superiority of single antiplatelet therapy with a P2Y12 inhibitor vs. dual antiplatelet therapy with a P2Y12 inhibitor and aspirin for the outcome of ISTH major or CRNM bleeding
The AUGUSTUS trial has two limitations:1,2
- TTR for patients on VKA was modestly lower than in some RCTs for stroke prevention in patients with NVAF. For patients randomised to VKA, the proportion of TTR (INR 2–3) was 56%
- This trial was not designed to be large enough to detect potentially clinically important differences in less common but important individual ischaemic outcomes
What was the study design?
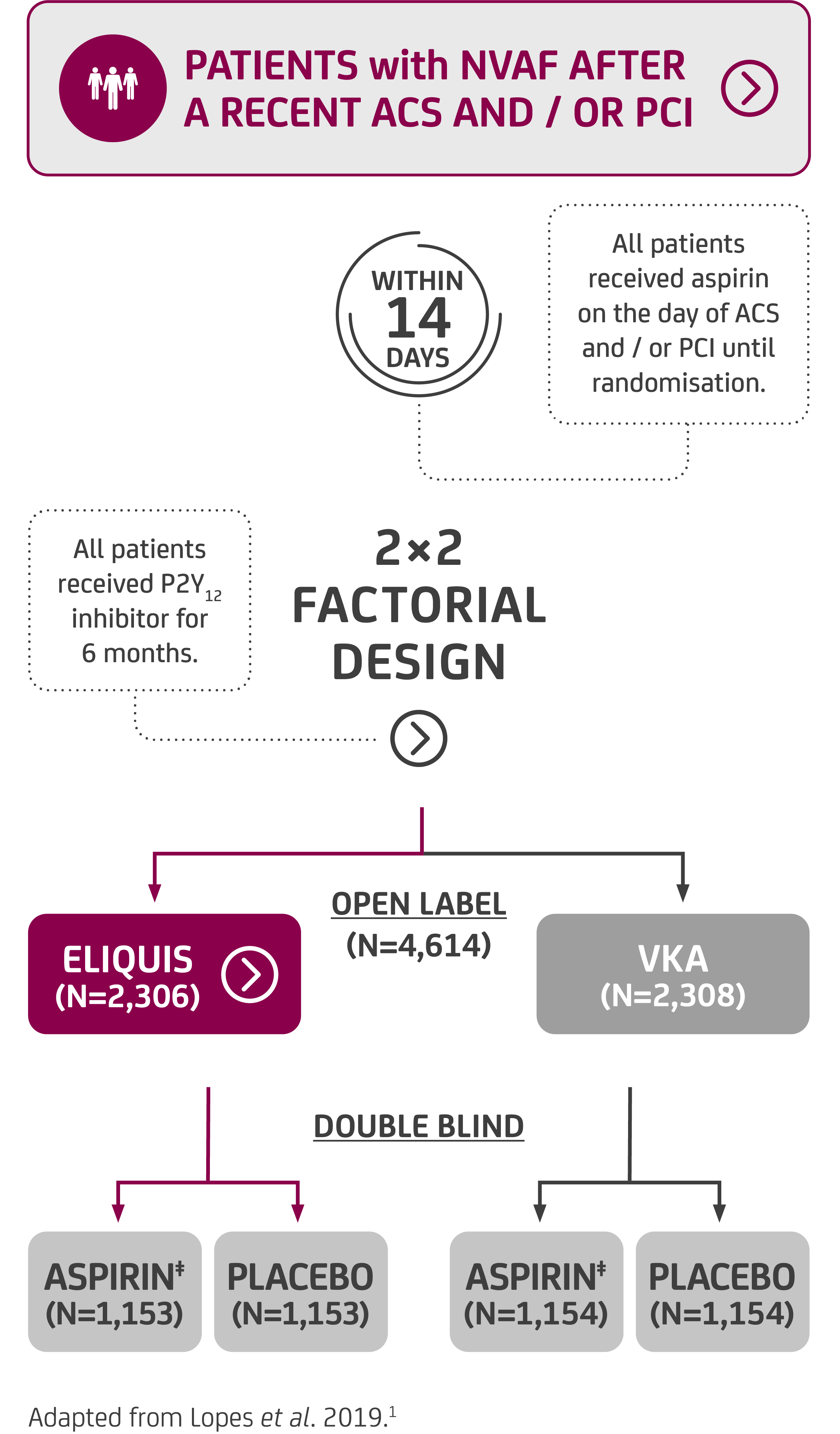
Patients with NVAF were randomised to the trial within 14 days of ACS and / or PCI and, by using a 2 x 2 factorial study design, investigators were able to test two interventions in one patient population.1
The recommended dose of ELIQUIS 5 mg BD was used unless the patient met two or more of the ABC dose reduction criteria (age ≥80 years, body weight ≤60 kg, creatinine ≥1.5 mg/dl [133 μmol/l]) in which case the reduced dose, ELIQUIS 2.5 mg BD, was used.1
Patients with severe renal impairment (CrCl 15–29 ml/min) alone should receive the ELIQUIS 2.5 mg BD reduced dose.2
ELIQUIS is not recommended in patients with CrCl <15 ml/min or in patients undergoing dialysis.2
What clinical endpoints were investigated?
At 6 months
Primary safety endpoint1
- Major bleeding or clinically relevant non-major bleeding§
Secondary efficacy endpoints1
- Composite of death or hospitalisation
- Composite of death or ischaemic events
(Stroke, myocardial infarction, definite / probable stent
thrombosis or urgent revascularisation)
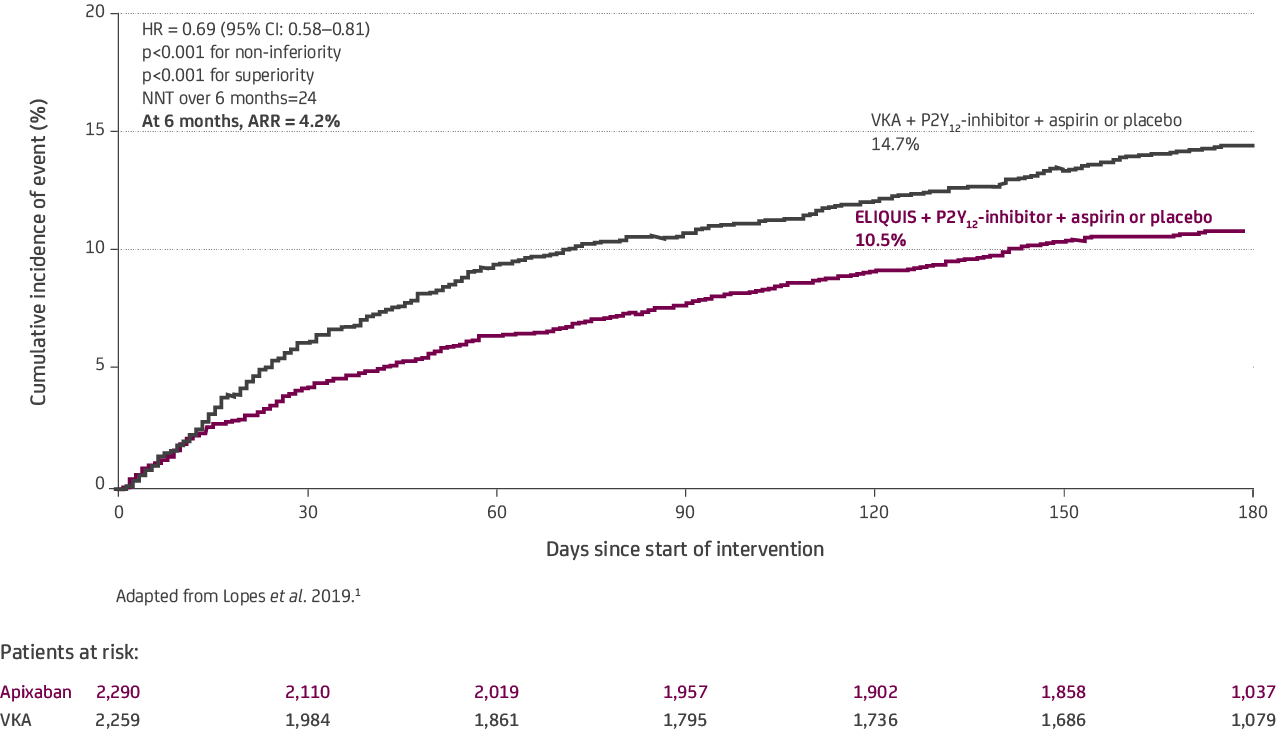
What were the major / CRNM bleeding outcomes?
Patients with NVAF were randomised to the trial within 14 days of ACS and / or PCI and, by using a 2 x 2 factorial study design, investigators were able to test two interventions in one patient population.1
Patients on ELIQUIS experienced significantly fewer major or CRNM bleeds vs. VKA1
- The primary safety endpoint, ELIQUIS showed overall superiority to VKA in the study population. For VKA, additional analyses using subgroups by TTR showed highest bleeding associated with the lowest quartile of TTR and similar bleeding rates in the highest quartile of TTR, vs. ELIQUIS2
- ELIQUIS should be used with caution when co-administered with aspirin and / or P2Y12 inhibitors because these medicinal products typically increase the bleeding risk2
- In patients with atrial fibrillation and conditions that warrant mono or dual antiplatelet therapy, a careful assessment of the potential benefits against the potential risks should be made before combining this therapy with ELIQUIS2
- Event rate per 100 patient-years
24.7 with ELIQUIS (n=241) vs. 35.8 with VKA (n=332), HR=0.69 (95% CI: 0.58-0.81); p<0.001
Refer to the ELIQUIS SmPC for further information.2
Patients on ELIQUIS experienced significantly fewer deaths or hospitalisations vs. VKA1
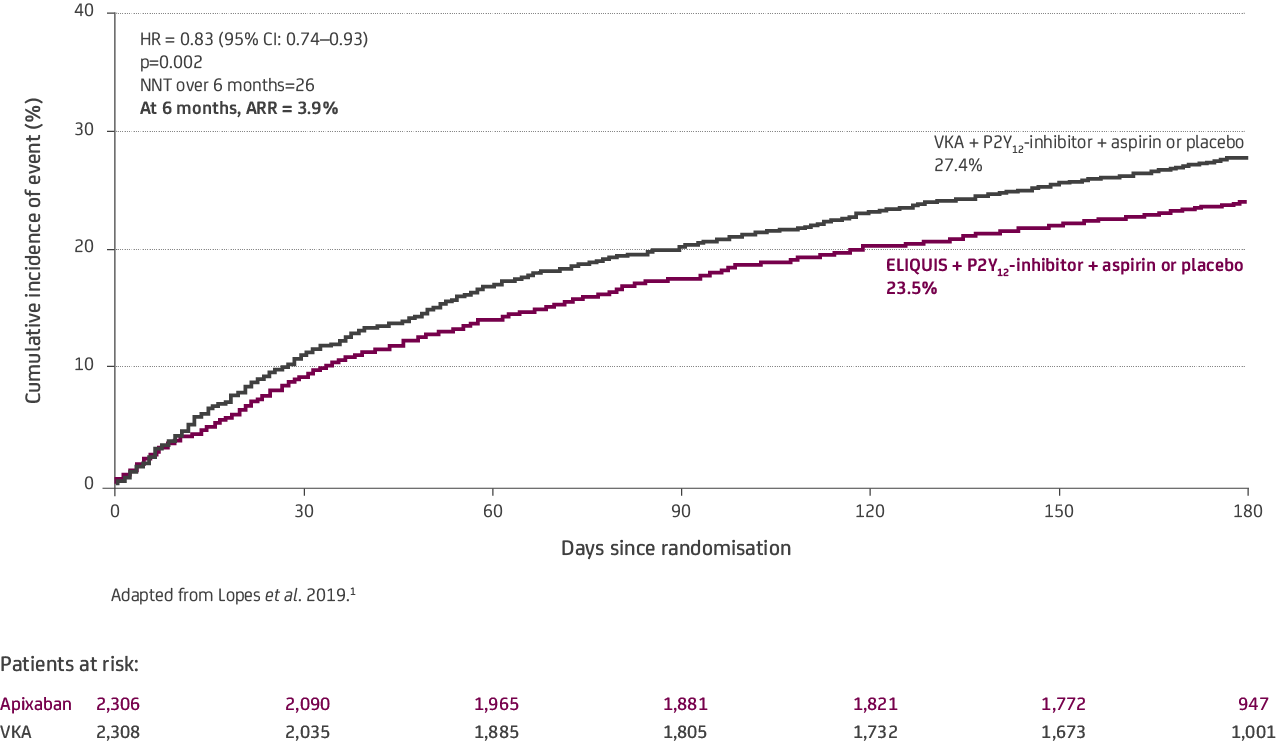
Event rate per 100 patient-years
57.2 with ELIQUIS (n=541) vs. 69.2 with VKA (n=632), HR=0.83 (95% CI: 0.74–0.93); p<0.0021
There was no significant difference in the incidence of death or ischaemic events between ELIQUIS and VKA.1
Event rate per 100 patient-years
14.3 with ELIQUIS (n=154) vs. 15.3 with VKA (n=163), HR=0.93 (95% CI: 0.75–1.16); p=NS1
Patients on aspirin experienced significantly more major or CRNM bleeds vs. placebo1
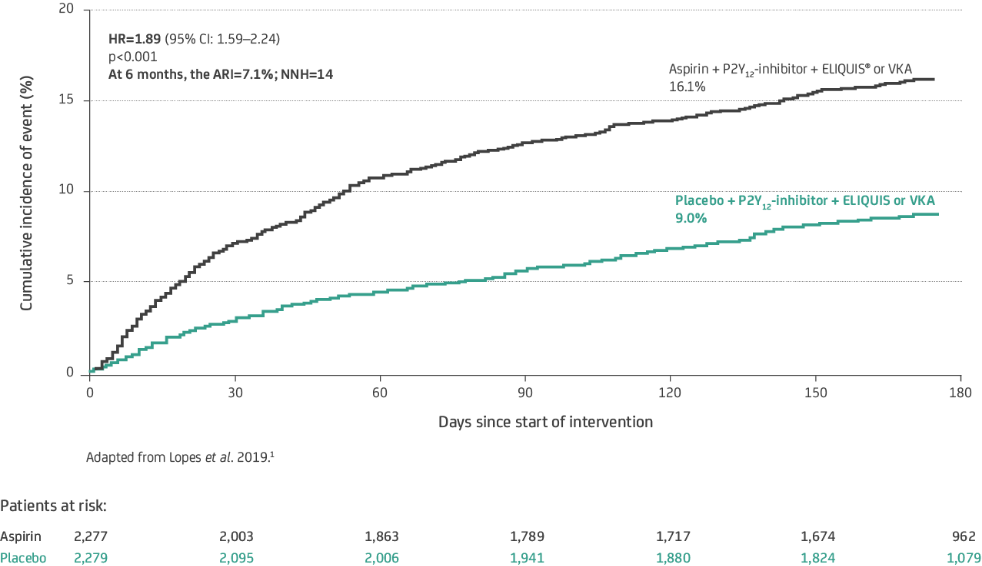
Event rate per 100 patient-years
40.5 with aspirin (n=367) vs. 21.0 with placebo (n=204), HR=1.89 (95% CI: 1.59–2.24); p<0.001 for superiority1
Patients on aspirin experienced no benefit in all-cause death or hospitalisation vs. placebo1
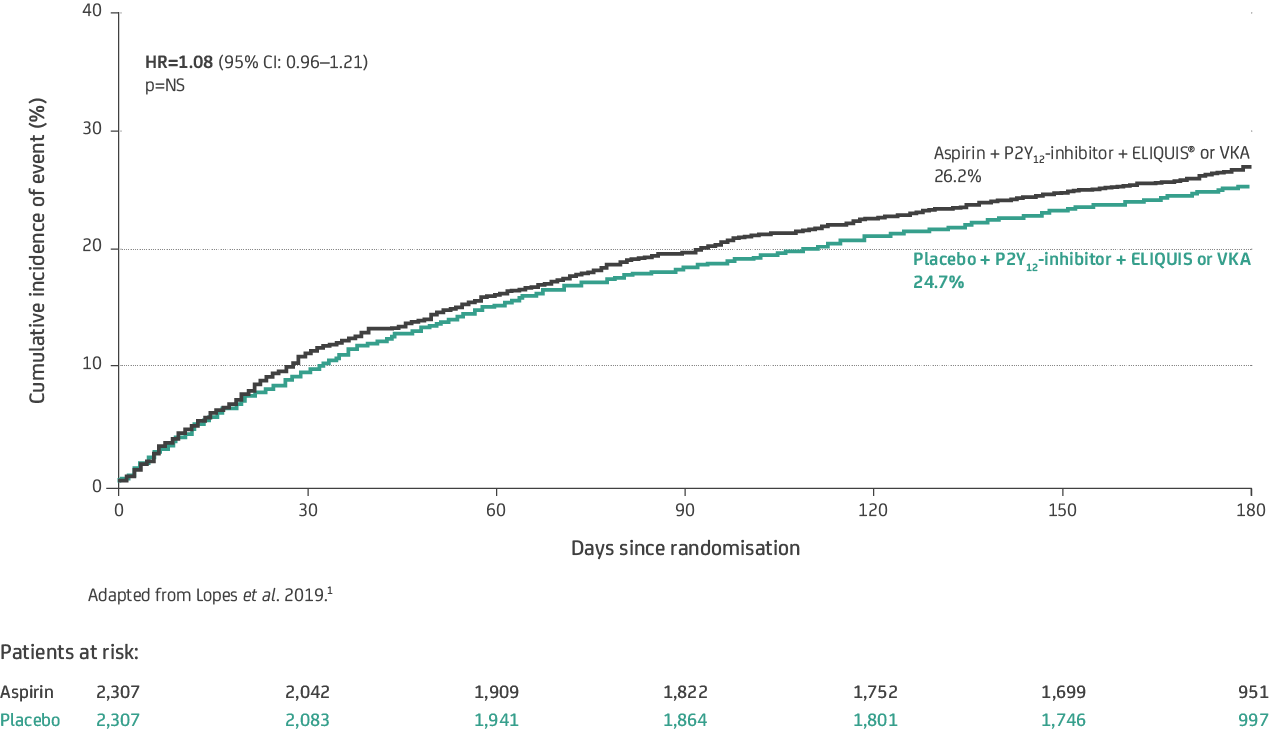
Event rate per 100 patient-years
65.7 with aspirin (n=604) vs. 60.6 with placebo (n=569), HR=1.08 (95% CI: 0.96–1.21); p=NS1
There was no significant difference in the incidence of death or ischaemic events between aspirin and placebo; however, more ischaemic events occured in the placebo group.
Event rate per 100 patient-years
13.9 with aspirin (n=149) vs. 15.7 with placebo (n=168), HR=0.89 (95% CI: 0.71–1.11); p=NT1
AUGUSTUS provides further data on the safety outcomes of ELIQUIS in patients with NVAF after a recent ACS and / or PCI.1
ELIQUIS (apixaban) is indicated for prevention of stroke and systemic embolism in adult patients with non-valvular atrial fibrillation (NVAF), with one or more risk factors, such as prior stroke or transient ischaemic attack (TIA), age ≥75 years, hypertension, diabetes mellitus, symptomatic heart failure (NYHA Class ≥II); treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE), and prevention of recurrent DVT and PE in adults; and, prevention of VTE in adult patients who have undergone elective hip or knee replacement surgery.2
Footnotes:
- * The AUGUSTUS clinical trial was a two-by-two factorial, randomised, controlled clinical trial in 4,614 patients who had an ACS or had undergone PCI. Patients were randomly assigned to receive open-label ELIQUIS 5 mg BD (or 2.5 mg BD in selected patients [10.0%]) or a VKA and to receive double-blind aspirin (81 mg) or matching placebo OD. The primary outcome for both factorial comparisons was major or CRNM bleeding as defined by the ISTH. Secondary outcomes included the composite of death or hospitalisation and the composite of death or ischaemic events (stroke, myocardial infarction, definite or probable stent thrombosis, or urgent revascularisation).1
- † This link is to a third-party site unaffiliated with the Pfizer / BMS Alliance. Please abide by the terms of use of the site.
- ‡ Aspirin was administered at a dose of 81 mg OD.
- § Major and clinically relevant non-major bleeding were defined according to the ISTH.1
- ACS = Acute Coronary Syndrome ARR = Absolute Risk Reduction BD = Twice Daily CI = Confidence Interval CRNM = Clinically Relevant Non-Major HR = Hazard Ratio ISTH = International Society on Thrombosis and Haemostasis NS = Not Significant NSAID = Non-Steroidal Anti-Inflammatory Drug NT = Not Tested NVAF = Non-Valvular Atrial Fibrillation OD = Once Daily PCI = Percutaneous Coronary Intervention P2Y12 = Purinergic signalling receptor Y12 SmPC = Summary of Product Characteristics TTR = Time in Therapeutic Range VKA = Vitamin K Antagonist
References:
- Lopes RD et al. N Engl J Med 2019; 380: 1509–1524.
- ELIQUIS® (apixaban) Summary of Product Characteristics
Reporting of suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via HPRA Pharmacovigilance at www.hpra.ie
Adverse reactions should also be reported to Bristol-Myers Squibb Medical Information on 1 800 749 749 or medical.information@bms.com